Meet the Middleman’s Middleman – KFF Health News
Some people who expected their health insurance to cover some out-of-network care have been getting stuck with enormous bills.
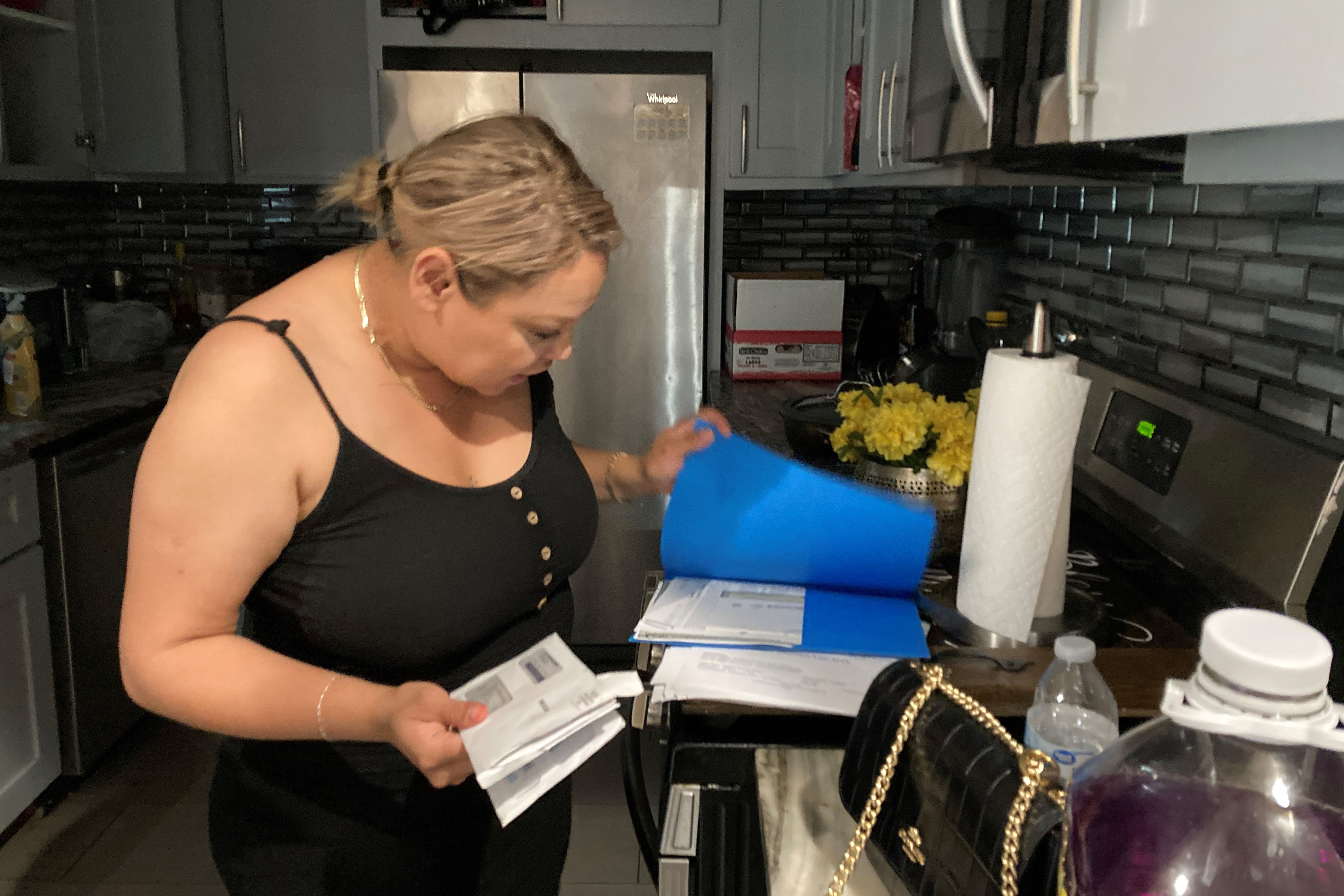
One Kansas City, Kansas, couple paid thousands of dollars out-of-pocket and up-front for care. They expected to get a partial reimbursement from their insurer. So, they were shocked when instead they got a bill saying they owed even more than what they’d already paid.
It turns out, a little-known data firm called MultiPlan was working with their insurance company to suggest cuts to their coverage. MulitPlan says it’s helping control ballooning health care costs by keeping hospitals and providers from overbilling. But it’s often patients left paying the difference.In this episode of “An Arm and a Leg,” host Dan Weissmann breaks down this confusing world of out-of-network care with New York Times reporter Chris Hamby, who recently published an investigation into MultiPlan.
Dan Weissmann
Host and producer of “An Arm and a Leg.” Previously, Dan was a staff reporter for Marketplace and Chicago’s WBEZ. His work also appears on All Things Considered, Marketplace, the BBC, 99 Percent Invisible, and Reveal, from the Center for Investigative Reporting.
Credits
Emily Pisacreta
Producer
Claire Davenport
Producer
Adam Raymonda
Audio wizard
Ellen Weiss
Editor
Click to open the Transcript
Transcript: Meet the Middleman’s Middleman
Note: “An Arm and a Leg” uses speech-recognition software to generate transcripts, which may contain errors. Please use the transcript as a tool but check the corresponding audio before quoting the podcast.
Dan: Hey there! Paul and Kristin live in Kansas City with their two kids. Kristin and their daughter, the older kid– they have some complex medical issues, need to see some specialized folks. And some of those folks don’t take Kristin and Paul’s insurance. They’re “out of network,” so Kristin and Paul pay out of pocket– a lot. Maybe $20,000 a year. BUT their health insurance plan does reimburse some out-of-network care.
o, in January 2023, Kristin called a help line connected with the insurance plan to find out how that was gonna work.
Kristin H: They basically said, sure, easy peasy, you pay and then you get online and you click this form, you show what you paid, and then we send you a check and reimburse you.
Dan: Kristin was on it. She built a whole spreadsheet to track every bill she paid, every reimbursement form she’d submitted. And she waited for the checks. The insurance company gave itself months just to process the claims. And when they finally sent statements, the statements seemed … weird. They were like:
Kristin H: Here’s what you paid, and here’s your discounts, and here’s what you may owe.
Dan: And Kristin was like … what?
Kristin H: Because I was thinking, well, I don’t owe anything. We paid out of pocket, but then I was thinking, well, this must be the portion that they’re paying us back. But then the math didn’t add up.
Dan: Yeah. Not at all. Kristin was expecting to get 50 percent back, like her plan said she would. But this amount wasn’t anything like 50 percent. And what’s this “discount” business?
It took months– and a lot of digging from Paul, and ultimately a talk with a NewYork Times reporter– before Kristin and Paul understood what was going on, and why it was costing them thousands of dollars.
What they didn’t know until that New York Times story came out was: Someone was making a multi-billion dollar business out of experiences like theirs. As that story made clear, LOTS of people who expected their insurance to cover them for expensive out-of-network care ended up on the hook for a lot more than they’d expected.
That story introduced readers to a character who’s become kind of a TYPE on this show. Not a type of person, but a type of business: A middleman that works behind the scenes with insurance companies. So we’ve seen that dynamic with pharmacy benefit managers– the folks who decide what drugs you can get and for how much– and more recently, we looked at a company that uses an algorithm to justify kicking folks out of nursing homes. The middleman in this New York Times story was a company called MultiPlan.
Reporter Chris Hamby found MultiPlan and insurance companies they worked with were leaving patients on the hook for huge amounts that they absolutely had not expected to pay. MultiPlan was also, along with those insurance companies, pocketing big fees. That story got some folks’ attention. A U.S. Senator has called for action from antitrust regulators. Those regulators might get interested. And we may wanna egg them on– so we’re gonna need to understand the whole scheme. Whothis middleman is– MultiPlan– and how they got themselves in the middle of 60 million people’s health insurance, by their own estimate … and how they make a lot of money.
This is An Arm and a Leg, a show about why health care costs so freaking much, and what we can maybe do about it. I’m Dan Weissmann. I’m a reporter, and I like a challenge. So, our job on this show is to take one of the most enraging, terrifying, depressing parts of American life– and bring you a show that’s entertaining, empowering, and useful.
And this time, I’ve got help.
Chris Hamby: My name is Chris Hamby. I’m a reporter on the investigations desk at the New York Times.
Dan: Yeah, and of course, Chris is the one who spent months figuring out the story of this middleman company, MultiPlan.
Chris Hamby: I was poking around a number of areas related to health insurance, and this name just kept coming up.
Dan: Like in lawsuits.
Chris Hamby: And it wasn’t always terribly clear what they did exactly or how they were compensated.
Dan: Or how doctors and patients– regular people– were affected.
Chris Hamby: So that’s why I decided to try and figure this out, and it’s sort of an opaque space as so many areas of health care are these days.
Dan: Yeah. In fact, in order to understand this story at all– to understand who’s doing WELL in this scenario– we’ve gotta peel back a layer. It’s something we’ve talked about here before, but not for a while, and you know, not even my mom remembers everything I’ve ever said here.
This is about the mechanics of how most health insurance people get from their job actually works: about who actually pays medical bills when your insurance settles a claim. It’s not the insurance company. It’s actually the employer paying those bills.
Of course, employers don’t know how to actually RUN an insurance plan. [Unless the employer is Aetna, I guess]. So they hire insurance companies to administer them. You get a card that says Cigna or Blue Cross, but your employer’s funds actually pay the medical bills, so these are called “self-funded” plans. But this is all stuff most of us are just not aware of.
Here’s Chris Hamby:
Chris Hamby: I hadn’t, until about a year ago, even heard of a self-funded plan. And I like to think that I’m reasonably well informed on this stuff.
Dan: Yeah, that is putting it mildly. Chris made his name and won a Pulitzer Prize covering workplace health issues. So, just park that for a minute: self-funded plan, where the employer is the “self,” actually paying the bills, and paying the insurance company a fee. The insurance company is a middleman.
OK, now, next layer: The middleman’s middleman. In this case, the company MultiPlan that Chris wrote about. What’s their job? So in this story, the job they’re doing– their middleman job– is to address what is admittedly kind of a tough question: If you go see somebody– a doctor, a therapist– who doesn’t take your insurance, what happens?
Chris Hamby: How do you determine what a fair amount to pay the provider is? And by extension, how much is the patient potentially on the hook for the unpaid balance? And that has long been a contentious issue.
Dan: Because, if they don’t take your insurance, a provider could charge … absolutely anything. So is your insurer– and again, that’s often actually your employer– supposed to pay absolutely anything? How much are they supposed to pay? Figuring that out, it’s a job.
About 15 years ago, another middleman company doing that job got sued by the NewYork state attorney general. The state said this earlier middleman’s way of figuring out what to pay was screwing over both providers and patients. And the state’s lawsuit produced a solution.
Chris Hamby: The insurance companies agreed to fund the creation of a nonprofit entity that was going be sort of an independent, neutral arbiter of fair prices. It was going to collect data from all the insurers and just make it publicly available. Make sure it was transparent to everyone.
Dan: This nonprofit is called FAIR Health, and its data is actually public. It still exists. Like, you can use it yourself — you can look up the going rate for a knee replacement, a blood test, whatever.
Chris Hamby: You can plug in your zip code, plug in your medical procedure and see an estimate of what, you know, typical out-of-network charges and in-network charges would be for these.
Dan: It’s cool! Check it out yourself; it’s useful. And all the major insurance companies agreed to use it– to use FAIR Health’s benchmarks– to decide what to pay for out-of-network stuff. But, those agreements only committed insurance companies to using FAIR Health for … five years. They expired in 2014.
Enter middleman companies like MultiPlan, saying to insurance companies: Hey, you COULD use FAIR Health– or you could route out-of-network bills to us: Hire us to get you an even better deal– better prices.
Chris Hamby: And it’s important to note also that this is a time when private equity is investing in healthcare, and there are some legitimate concerns about driving up those list prices to ridiculously high levels in a lot of cases. So, there were real issues that insurers were saying that they were responding to at the time.
Dan: OK, so that’s the pitch. MultiPlan is saying to insurance companies: We’ll help you hold the line. We can save you more money than if you used FAIR Health. Well, kind of. Because here’s where we come back to the whole thing about self-funded insurance. MultiPlan isn’t saying, “We can save YOU, insurance company, more money than if you used FAIR Health.” They’re saying, “We can help you save your CLIENTS– employers who do self-funded health insurance– more money. And when you save them money, you’re gonna make money. Because you can charge them a percentage of what you’re saving them. And we’ll get a percentage too.” A percentage of the savings. On every single bill. That’s a very different deal than just using FAIR Health’s data.
Chris Hamby: FAIR Health is not taking a percentage of the savings that they obtain. They’re just selling you their data. And the insurers typically are not charging employers a fee for using FAIR Health’s data. But if they use MultiPlan’s data, both MultiPlan and the insurer typically charge a fee.
Dan: A percentage. In examples from Chris’s story, the insurance company gets 35 percent of those savings.
Chris Hamby: And this has become a significant amount of money for a lot of insurance companies. Overall, UnitedHealthcare, is up to, you know, around a billion dollars per year in recent years.
Dan: UnitedHealthcare collects like a billion dollars in fees for these services, basically, for using MultiPlan specifically?
Chris Hamby: And they couch that by saying some other out-of-network savings programs, but yes.
Dan: Whooh!
Chris Hamby: One thing that the insurers say is that the employers are aware of this; they’ve signed up for it.
Dan: That employers are hiring, say, Cigna, with MultiPlan to find savings. And employers are agreeing to the fees.
Chris Hamby: Where it gets a little bit dicier from the employer’s perspective is when you see claims where, for instance, you end up paying the insurance company more in fees than you paid the doctor for treating your employee.
Dan: yeah, one example from Chris’s story: An out-of-network provider wanted more than $150,000 on one bill. And after the insurance company and MultiPlan did their bit, the employer, a trucking company, ended up paying $58,000. Eight thousand for the provider, and $50,000 to the insurance company and MultiPlan. So, on the one hand, the employer maybe saved $90,000. But paying $50,000 for “cost containment?” Maybe doesn’t sound like such a bargain.
Some employers and a union that runs a health plan have filed lawsuits looking for some of that money back. And there’s also a big irony here because MultiPlan’s pitch is, you need us because sticker prices are super-wildly high. But MultiPlan isn’t doing anything to contain the sticker prices as a systemic problem. In fact, the higher providers crank up their sticker prices, the more money MultiPlan and the insurance companies they work with can make. But then there’s a big question too, which is, what happens to the rest of that bill for the sticker price? Who pays that? That’s next …
This episode of An Arm and a Leg is a co-production of Public Road Productions and KFF Health News. The folks at KFF Health News are amazing journalists. Their work wins all kinds of awards, every year. We’re honored to work with them.
So, a provider sends a bill. MultiPlan and the insurance company say, “Woah, way too much.” And then what happens? Well, it depends. Sometimes, MultiPlan negotiates with the provider. They’ve got people who do this. And those negotiators drive hard bargains. According to Chris’s story, negotiators sometimes tell providers: Here’s my offer, you’ve got a few hours to take it or leave it, and my next offer might be lower.
Chris talked with a pediatric therapist who said an offer based on MultiPlan’s calculation was less than half of what Medicaid pays. Less than half. And Medicaid rates– they’re notoriously pretty low. Chris talked with some of MultiPlan’s negotiators too.
Chris Hamby: It was interesting because some of the negotiators felt that they were doing their part to hold down costs and really sort of stick it to providers and hospitals that were price gouging.
Dan: But …one told Chris she knew the offers she made– they weren’t fair. “It’s just a game,” another one said. “It’s sad.” And maybe the difference is that some of these negotiators were thinking of a big hospital charging $150,000 for something. And maybe some of them were thinking of someone like that therapist– the one who got offered less than half of Medicaid’s rate.
And I’m not gonna get into the question of who should be doing this kind of negotiating, or what’s fair. I mean, not today, anyway. Because: in a lot of cases with MultiPlan, there’s no negotiation at all. Negotiation only happens when the employer has told the insurance company, look, protect my people. Figure out SOMETHING with the provider so they don’t go after my workers for the rest.
But that doesn’t always happen. A lot of the time, what happens is: The provider sends a bill. The insurance company kicks in whatever it decides to … and that’s it.
So Chris’s story opens with a woman who had surgery. With MultiPlan’s help, her insurance company decided to pay about $5,400. And she got stuck with a bill for more than $100,000.
And then there’s Kristin and Paul in Kansas City. They paid their bills upfront and then looked to get reimbursed– kept a spreadsheet. But when their claims finally got processed, the numbers didn’t add up. Here’s what they saw: Like pretty much every insurance plan, Kristin and Paul’s had a “deductible”– an amount they had to pay out of pocket before insurance would reimburse anything.
Kristin H: Then I started watching the deductible and you know, when I calculated my spreadsheet of how much we had paid out of pocket, and when we saw what was on like our out-of-network spend, those two weren’t matching.
Dan: She really couldn’t figure this out.
Kristin H: I just kind of handed over all of my spreadsheets to Paul, and so that’s when he started digging into the “your discount.”
Dan: “Your discount…” That was this mysterious number on all the statements from the insurance company. In addition to the provider’s rate, and what insurance might pay, the statements listed, quote, “your discount.”
Paul H: And I’m like, what is this? I don’t understand why it’s talking about a discount. We are paying cash out of pocket to the provider at their billed rate, and our insurance is saying that there’s some sort of discount.
Dan: After a bunch of phone calls, he figured it out: The discount was … the difference between the amount on the bill and what the insurance company– with MultiPlan’s help– had decided was a “fair price.”
Paul H: For example, an occupational therapy bill that might be $125, this third party adjuster might come back and say, essentially what the market rate for that should be is $76. And so, your discount, quote, unquote, is $49.
Dan: Except of course, it wasn’t a discount for Kristin and Paul. They had already paid that $49, when they paid the provider upfront. Once Kristin and Paul learned what the “discount” actually meant, they started to understand who actually got the benefit– the insurer. Because …
Kristin H: That discounted rate is actually what will be applied to your deductible. So you’re not going to hit your deductible nearly as quickly as you think. Right? Because we’ve essentially ignored half of your payment.
Dan: This hits Kristin and Paul in two ways.
First, it means they’re actually spending a lot more before their insurance kicks in. It also means that when their insurance does start reimbursing them a percentage of what they’ve spent, the insurance is only paying a percentage of that lower amount. Overall, it means the reimbursements Kristin and Paul get are gonna be thousands of dollars less than they’d expected.
I mean, it took a LOT of work for Kristin and Paul to figure this out. At one point, Paul posted to Reddit asking for help– that’s where Chris Hamby found him. In Paul’s post, he noted how nobody ever even mentioned this third-party adjuster– not until he had already talked to his insurance company for what he said was “about 18 times.” Frequently on hold for 45 minutes or more.
Kristin says once they finally figured out what was going on, they could figure out how to budget for it. There were sacrifices. She stopped seeing one of her providers as often. But finally figuring out what was going on also allowed them to live with it.
Kristin H: The infuriating part was telling, like doing exactly what we were told to do, following the process, and then feeling like you are crazy. Like why, why doesn’t this make sense? You know? And so I think I’m fortunate that Paul just wouldn’t let it die and was gonna research until he figured it out.
Dan: You did all of the work, you tracked it down, you identified the problem, and you, as you say, kind of resigned yourself to it. You’re like, okay, this Goliath is not– we don’t have the slingshot for this. Goliath is stomping all over our town, and we have to live in that reality. Having the knowledge, having done that work, gives you, it sounds like, an ability to have some peace. Like having tracked it down means that this sucks, but it’s not the same as living in a situation where like, now what? Like anything could happen.
Kristin H: Yeah, you feel crazy or hopeless. You know? Like I’ve done everything and this doesn’t … So there’s just the sense of like, am I missing something? You know, is there anything left for me to do? I recognize that everyone is not like this, but for me, knowledge is a gift.
Dan: Chris Hamby says there’s rarely a way to get this kind of knowledge in advance. He says you’re unlikely to find these kinds of details in your insurance plan document.
Chris Hamby: It typically will not say when you go out of network, we’re going to send your claim to a third party that you’ve never heard of to price it. It will just give some sort of vague language about competitive rates in your geographic area. And if you call up in advance of seeking the care to try and get an estimate, most of the time you will not get much more specifics than that. They tell you you have to just go and they’ll process the claim and you’ll see when the explanation of benefits comes through.
Dan: Yeah, and look, I hate to get you even angrier, but Chris says the rules can change on you, without notice.
Chris Hamby: A lot of people that I talk with also have seen no change in their insurance plan, but they’ve seen their reimbursement rates decline over time.
Dan: Turns out, behind the scenes, their insurance made a switch from a service like FAIR Health, which looks at what’s getting paid in general, to a service like MultiPlan, which looks for the steepest possible price cuts.
Chris Hamby: And the difference between those two amounts can be vast. So you have people who in some cases stop seeing their doctors because their costs doubled almost overnight.
Dan: Oh god. And still. Better to know. Better that as many of us know as possible. That’s why Chris reviewed more than 50,000 pages of documents, and interviewed more than a hundred people for that story. And why lawyers for the New York Times helped get courts to agree to give him documents that had been under seal.
Kristin and Paul– who had figured most of this out for themselves– they definitely appreciated all that work.
Paul H: When Chris published the article that he did, it was very validating to know we’re not the only ones who are in this same boat. And there’s actually people who have had far worse experiences than ours. Like, ours kind of pale in comparison. And then immediately, like, within 24 hours to see 1,500 or 1,600 comments on the article talking about it. It’s like, okay, I might not have the stone that can slay the giant, but maybe The NewYork Times has the right sling and they might have the right stone to at least start the conversation.
Dan: A few weeks after Chris’s article came out, U.S. Senator Amy Klobuchar sent the top federal antitrust regulators a letter: She wanted them to take a hard look at MultiPlan.
Chris Hamby: She expressed concern about the potential for price fixing here.
Dan: Actually, Chris says some providers have already filed lawsuits against MultiPlan based on antitrust allegations.
Chris Hamby: The idea is that all the insurance companies outsource their pricing decisions to a common vendor. They’re essentially fixing prices via algorithm is the allegation.
Dan: As we noted here a few episodes ago, these antitrust regulators in the Biden administration have gotten pretty feisty. [That was the episode about the cyberattack on a company called Change Healthcare. It was called “The Hack,” if you missed it. Pretty fun!]
And I mean, those antitrust regulators have their work cut out for them. And a lot of targets. But I do want to egg them on here. I suspect you do too. Meanwhile, you’re egging US on.
Listener 1: The first thought that went through my head was I’m going to fight this because this is absolutely ridiculous. I’ve already paid for this.
Dan: A few weeks ago, we asked you for stories about your experiences with sneaky fees, often called facility fees.
Listener 2: When the facility fee is twice the office visit fee, it’s just crazy. I mean, it’s a 10-minute appointment for a prescription.
Dan: You came through, and now we’re making some calls, digging in for more details, and learning so much. We’re gonna have a sneak preview for you in a few weeks. Till then, take care of yourself.
This episode of An Arm and a Leg was produced by me, Dan Weissmann, with help from Emily Pisacreta and Claire Davenport– our summer intern. Welcome aboard, Claire!– and edited by Ellen Weiss. Adam Raymonda is our audio wizard. Our music is by Dave Weiner and Blue Dot Sessions. Gabrielle Healy is our managing editor for audience. Gabe Bullard is our engagement editor. Bea Bosco is our consulting director of operations. Sarah Ballama is our operations manager.
An Arm and a Leg is produced in partnership with KFF Health News. That’s a national newsroom producing in-depth journalism about healthcare in America and a core program at KFF, an independent source of health policy research, polling and journalism. Zach Dyer is senior audio producer at KFF Health News. He’s editorial liaison to this show.
And thanks to the Institute for Nonprofit News for serving as our fiscal sponsor, allowing us to accept tax-exempt donations. You can learn more about INN at INN.org. Finally, thanks to everybody who supports this show financially. You can join in any time at https://armandalegshow.com/support/
Thanks for pitching in if you can, and thanks for listening.
“An Arm and a Leg” is a co-production of KFF Health News and Public Road Productions.
To keep in touch with “An Arm and a Leg,” subscribe to its newsletters. You can also follow the show on Facebook and the social platform X. And if you’ve got stories to tell about the health care system, the producers would love to hear from you.
To hear all KFF Health News podcasts, click here.
And subscribe to “An Arm and a Leg” on Spotify, Apple Podcasts, Pocket Casts, or wherever you listen to podcasts.