The Host
Julie Rovner
KFF Health News
@jrovner
Read Julie’s stories.
Julie Rovner is chief Washington correspondent and host of KFF Health News’ weekly health policy news podcast, “What the Health?” A noted expert on health policy issues, Julie is the author of the critically praised reference book “Health Care Politics and Policy A to Z,” now in its third edition.
Incoming President Donald Trump’s inauguration is Monday, yet the new GOP-led Congress is already rushing to work his priorities into legislation, eyeing cuts to Medicaid to pay for new tax and immigration priorities. But even in its waning days, the Biden administration continues to make big policy moves, including a possible order for tobacco companies to dramatically decrease the amount of nicotine in cigarettes.
Meanwhile, the fires in Los Angeles are drawing new attention to the health dangers of not just smoke from organic matter, but also toxic substances released by burning plastic and other man-made materials — as well as the threat posed to both air and water quality.
This week’s panelists are Julie Rovner of KFF Health News, Anna Edney of Bloomberg News, Joanne Kenen of the Johns Hopkins University Bloomberg School of Public Health and Politico Magazine, and Sandhya Raman of CQ Roll Call.
Panelists
Anna Edney
Bloomberg
@annaedney
Read Anna’s stories.
Joanne Kenen
Johns Hopkins University and Politico
@JoanneKenen
Read Joanne’s stories.
Sandhya Raman
CQ Roll Call
@SandhyaWrites
Read Sandhya’s stories.
Among the takeaways from this week’s episode:
- Republican lawmakers are weighing options to cut federal spending on Medicaid, the nearly $900-billion-a-year government program that covers 1 in 5 Americans. They could use the savings to bolster Trump priorities, such as extending the 2017 tax cuts. The GOP made splashy but unsuccessful attempts to cut Medicaid when Trump first took office and the party held a larger House majority — though the party seems more aligned with Trump today than it was then.
- Congress has gotten down to business on messaging bills: It advanced legislation this week that would ban trans athletes from girls’ school sports and, separately, a measure to detain and even deport immigrants who are living in the U.S. without legal status and have been charged with, though not convicted of, minor crimes such as shoplifting.
- The Supreme Court has agreed to hear a case later this year about the U.S. Preventive Services Task Force — an independent body of experts that issues recommendations in disease prevention and medicine. A ruling against its authority could strip coverage for key preventive health services from not just those with Affordable Care Act coverage, but also those on employer-sponsored health plans. The question stands: If not this task force, who would make the determinations about what preventive care should be covered?
- And the outgoing Biden administration issued a slew of health regulations this week, including a ban on the dye Red No. 3 in food and other ingested products, as well as an early regulation limiting the amount of nicotine in tobacco products. The incoming Trump administration could upend these and more regulations, though some do align with its policy interests.
Also this week, Rovner interviews Harris Meyer, who reported and wrote the latest KFF Health News “Bill of the Month” feature, about a colonoscopy that came with a much larger price tag than estimated. If you have a mystifying or outrageous medical bill you’d like to share with us, you can do that here.
Plus, for “extra credit,” the panelists suggest health policy stories they read (or wrote) this week that they think you should read, too:
Julie Rovner: KFF Health News’ “Can Medical Schools Funnel More Doctors Into the Primary Care Pipeline?” by Felice J. Freyer.
Anna Edney: Bloomberg News’ “It’s Not Just Sunscreen. Toxic Products Line the Drugstore Aisles,” by Anna Edney.
Joanne Kenen: The Atlantic’s “A Secret Way To Fight Off Stomach Bugs,” by Daniel Engber.
Sandhya Raman: Nature’s “New Obesity Definition Sidelines BMI To Focus on Health,” by Giorgia Guglielmi.
Also mentioned in this week’s podcast:
Click to open the transcript
Transcript: Hello, Trump. Bye-Bye, Biden.
[Editor’s note: This transcript was generated using both transcription software and a human’s light touch. It has been edited for style and clarity.]
Julie Rovner: Hello and welcome back to “What The Health.” I’m Julie Rovner, chief Washington correspondent for KFF Health News, and I’m joined by some of the best and smartest health reporters in Washington. We’re taping this week on Thursday, Jan. 16, at 10 a.m. As always, news happens fast and things might have changed by the time you hear this. So, here we go.
Today we are joined via videoconference by Anna Edney of Bloomberg News.
Anna Edney: Hi, everybody.
Rovner: Sandhya Raman of CQ Roll Call.
Sandhya Raman: Good morning, everyone.
Rovner: And Joanne Kenen of the Johns Hopkins Bloomberg School of Public Health and Politico Magazine.
Joanne Kenen: Hi, everybody.
Rovner: Later in this episode we’ll have my interview with Harris Meyer, who reported and wrote the latest KFF Health News “Bill of the Month,” about a patient whose colonoscopy bill was a lot bigger than he expected. But first, this week’s news.
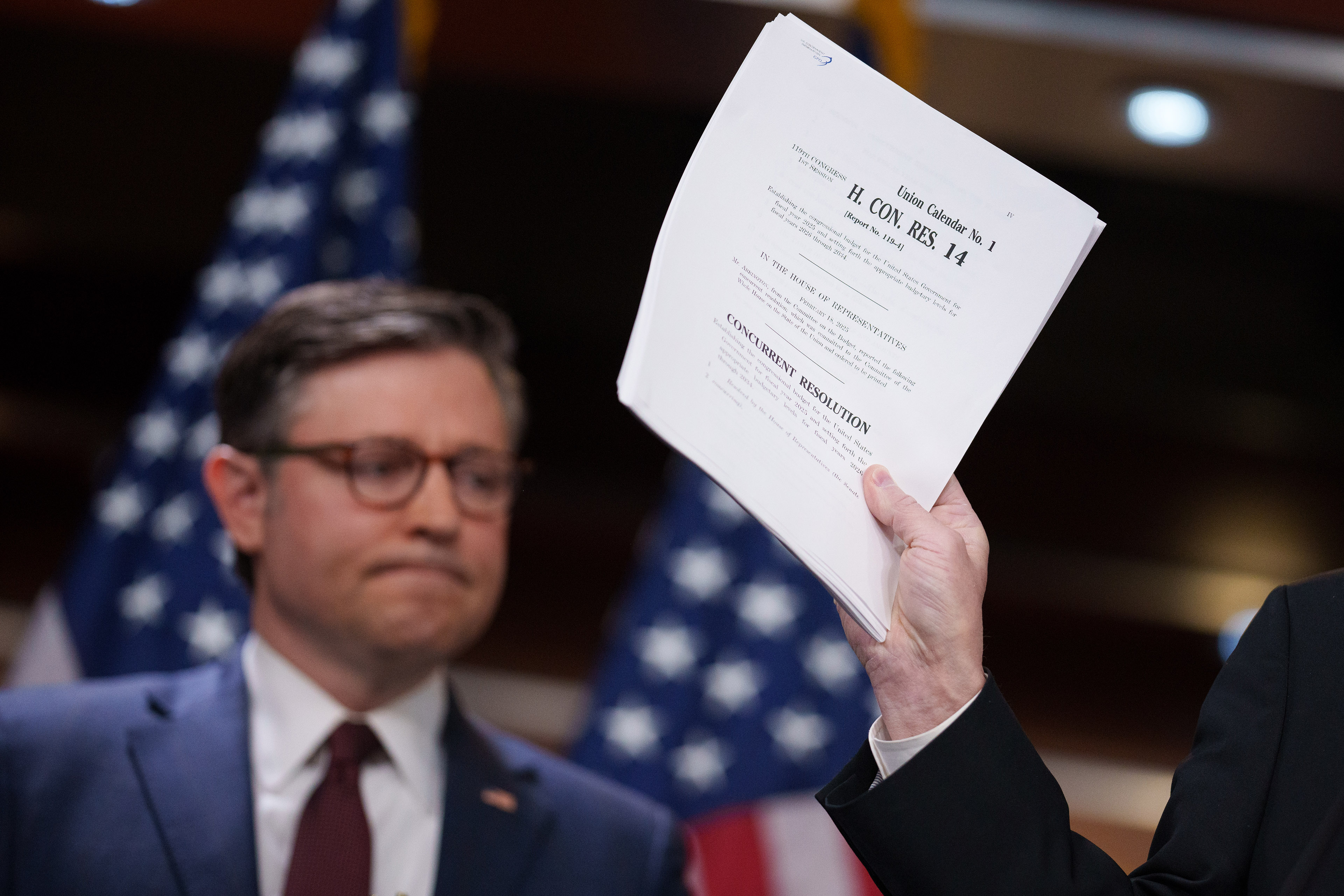
So we are now four days from the second swearing-in of Donald Trump as president, and discussions are already picking up on Capitol Hill about rolling the new president’s entire agenda into, quote, “one big, beautiful bill,” as Trump has put it. There are lots of differences of opinions between Republicans that are still to be worked out, but one target for cost-cutting is pretty clear, and that would be Medicaid. Sandhya, we’re starting to get a picture of the possibilities of how they might want to do that. What are some of the main things that are on the table?
Raman: So the reconciliation talks are very much underway, and we’ve made a little progress but at the same time we just didn’t also make a lot of progress. The end of, -ish, last week we got a menu of items that Republicans are kind of considering as things they would use to offset some of the things that they’d want to do through reconciliation.
Rovner: Like continue the tax cut?
Raman: Yes, for the tax cuts and for border security. So what we have on the House side is a lot of things that are very health-oriented. About half of that list is health-oriented, and a lot of it is Medicaid. And so some of the things they’ve been floating around are some things we saw in the first Trump administration, them trying to do. We have per-capita caps on Medicaid spending, work requirements for Medicaid, changing the federal match for Medicaid expansion, and things like changing the public charge rule to back how it was in the Trump administration.
Rovner: Remind people what the public charge rule is.
Raman: The public charge rule kind of limits some of the social programs for folks that are not citizens to make use of things like Medicaid, SNAP [the Supplemental Nutrition Assistance Program], and other programs like that.
Rovner: And those are for people who are here legally?
Raman: Yes. So this week, Tuesday, we had our first meeting from the House Energy and Commerce Republicans to look over at least the health part of that menu. And talking to both Energy and Commerce Chairman Brett Guthrie and Buddy Carter, who heads the health subcommittee, it’s just the start. Discussions were pretty good, but it’s so early.
Carter said that he still wants to get the PBM [pharmacy benefit manager] language from last year that didn’t make it across the finish line in there. And Guthrie has said that some of the numbers that we’ve seen of how much money from Medicaid they could possibly save are really in flux because of how they interact with all of the other provisions in there. Some things are under Ways and Means jurisdictions. Some things, if you do one and not the other, the numbers would change.
So they’re still pretty early in the process, and we don’t know if we’re going to do the “one big, beautiful bill” or kind of what the Senate wants, with two bills, and that would just kind of change what would be done earlier versus later. But we do have a little bit more of a timeline now in what they’re trying to do.
Rovner: I feel like it’s worth remembering that they tried taking a whack out of Medicaid in 2017, when they had a much bigger Republican majority in the House, and they couldn’t get it over the finish line. What makes them think they’re going to be more successful this time?
Raman: I think part of it is that — this is still early on. When you ask them the feedback that they’ve gotten from Republican governors — most Republican states have had Medicaid expansion at this point. We still have only the 10 holdout expansion states. So, I think, really, as we get closer, if they seem like they’re angling to include some of these in whatever vehicle we have, we’ll probably hear more.
And I mean, if you look at this state-level already, a lot of states are kind of couching their bets with Medicaid, just thinking about how they can do things differently in case their Medicaid federal funding changes over the course of this year or next year. So, I think it really depends on what feedback they’re going to get in the coming weeks and months.
Rovner: Joanne wanted to add something.
Kenen: Yeah, I mean, the beauty of reconciliation if you’re the majority party, but a narrow majority, which is what’s going on now, is you’d only need 51 votes in the Senate. You don’t need 60. So on one level, that sounds like they’ve got 53. It’s a slam dunk, right? But it’s not, because reconciliation, it’s a grab bag. You put so much stuff in there, and all you need is one provision that this person won’t vote for or that person won’t vote for.
So this seemingly simple slam dunk for a narrow-majority Senate is actually a big, complicated mess. On the other hand, compared to the first Trump administration, this is a more conservative, or a more populist, or a more approach — I mean, the ideology or worldview of the Republicans in Congress is closer to Trump than it was in 2017.
But yeah, they failed at what they thought was going to be easy. They thought repealing the ACA [Affordable Care Act] and changing, which included a lot of Medicaid stuff, they thought it was a slam dunk. And instead, it was a year-long slog that failed. So is Medicaid going to look the way it looks right now? No, it’ll change. How much will it change is really an open question.
Remember, there’s some things they can do through waivers. Work requirements they can do through waivers. Although in the past, the courts have blocked them. The courts have changed. We don’t know where the courts will come down. But really it’s more than a headache. It’s like a headache and a stomachache.
Rovner: Yeah, well, so reconciliation, budget, all of this stuff is still way TBD. Still, the Republican Congress is getting off to a fast start, at least in terms of messaging legislation. The House this week passed a bill to ban transgender athletes from women’s school sports, and the Senate’s debating a House-passed bill that would allow the deportation of undocumented people who are accused but not yet convicted of violent crimes.
In West Virginia, the new governor, who’s also a former Capitol Hill health aide, [Patrick] Morrisey, issued executive orders making it easier for parents to send their children to school without being vaccinated. Overall, it seems the Republicans are kind of coalescing around a concept known as “medical freedom,” which to me seems just like a rejection of public health in general. Or am I missing something? Is there something more to this?
Edney: No, I think that it’s always been around, but I think that certainly this resurgence in it is coming from the fact that people didn’t trust science during the pandemic. They were fed up. Communication wasn’t handled very well, and it still isn’t handled very well. I don’t think people have figured out how to talk about these things in measured ways.
I would recommend if someone listening hasn’t read, Dr. Paul Offit wrote an op-ed in the New York Times a few days ago on vaccination that I thought was really good because he’s like: Listen, I’m a vaccine skeptic. Like, R.F.K. Jr. [Robert F. Kennedy Jr.] is a vaccine cynic. There’s the difference, and here’s what it is. And he laid it out there. And he is a pediatrician, and he also serves on FDA’s [the Food and Drug Administration’s] advisory committee for vaccines.
So I think that a lot of this is stemming from misinformation and miscommunication, and it resonates with people. I mean, the Republican Party picked up a lot of fans in far-left progressives by talking about this. So I think they see that as an opportunity, too. So it may not just be grassroots. It may be a little bit of an opportunity they see.
Kenen: Anti-vaccination sentiment has been around as long as vaccines. It actually goes back to smallpox. There has always been a certain amount of fear, skepticism, whatever. It had been traditionally among Democrats and Republicans. It actually changed. It began to change two or three years before the pandemic.
Some state legislatures — and this was the medical freedom, this was on the right — started trying to water down mandates for schools. At that point, I don’t think anything big got through. But we began to see this emergence of a deeper politicization of vaccination. And it was on the right, and it’s what we now talk about as medical freedom.
So instead of being something that’s across the political spectrum, it is now a politicized movement, on a libertarian Government can’t tell me what to do. And we saw this during the pandemic. And neither administration, neither the Trump administration in the first year of the pandemic nor the Biden administration in the ensuing years, really managed to explain the difference between individual choice and the fact that if you get sick, you might survive but you could endanger somebody else.
You don’t know who the person on the bus next to you is. You don’t know who the kid in your classroom is. You don’t know who you’re standing next to at the grocery store. They could be really vulnerable. And that this whole sense of “my body, my choice,” doesn’t fly when you could kill somebody else unintentionally. And that sort of has been lost, or people don’t care.
Rovner: Yeah, I mean we’ve seen that with tobacco over how many generations. It’s like, you want to put stuff in your lungs, that’s your business. But you don’t really get the right to put stuff in other people’s lungs because you would like to smoke.
Meanwhile, continuing with the Republican agenda, my former KFF Health News colleague Anna Maria Barry-Jester has a really good story this week about what National Institutes of Health director candidate Jay Bhattacharya might have in mind for the agency, including de-emphasizing infectious disease research and focusing more on chronic disease.
Given that the biggest institute at NIH is already the National Cancer Institute, which focuses on a chronic disease, is this just Republicans’ way of punishing the National Institute of Allergy and Infectious Diseases that was for so long headed by the now retired Dr. Tony Fauci?
Raman: I think in a part that is a huge driving factor, when you look at some of his comments and R.F.K. Jr.’s comments about holistic approaches to health, that really when you look at what something like NIAID does, which is so infectious-disease-driven, versus the things like with cancer and other things.
But I think at the same time, this has kind of been bubbling up before, when we even looked to last year. Before we had any of these nominees, before we even knew the outcome of the election, we had a push within Congress from the head of the House Labor-H Appropriations subcommittee and former Energy and Commerce Chairwoman Cathy McMorris Rodgers trying to reform NIH that way.
We didn’t get that far with it. It was included in some of the appropriations bills that didn’t go anywhere yet. But I think it’s just part of a broader discussion that there is, kind of going back to what we were saying before, some of the wanting more control of what you see, in terms of medical freedom, and that they want to know more about what’s happening.
So I think that, regardless, we’re going to see more of this. But I think one thing that was really interesting in what she’d been writing was just the NIH is so much bigger than just NIH, you know? It’s so many of the people that are benefited by it, that are working with this grant money, are states nationwide. And it’s just the medical research is for a global understanding of medical research, and just how many of the drugs that we see come from NIH money. So even if there is a broader push for reform, that it’s very sensitive into how broad of an effect that would have.
Rovner: And I would point out, because I live up the street from NIH, that most of what NIH does doesn’t happen on the NIH campus. It is, as you said, it’s money that goes out to every single congressional district. There’s an enormous amount of backing.
I would also point out that, yes, NIH has gotten kind of sprawling with, I think there’s 27 institutes now. Every single one of those has been added by Congress. NIH can’t create its own institutes. Only Congress can do that. So, Congress has sort of made NIH the sprawl that it is. I think there’s been bipartisan agreement that NIH maybe needs a new look.
I guess the question is just sort of what direction that is going to take and whether some of it is going to be punitive or whether they’re actually going to look at it in a matter of what would benefit the country, because it gets a lot of money, and that’s also been bipartisan.
Kenen: Right. What we’re not hearing yet, or at least — and maybe Anna, who covers pharma, can tell me if I’m wrong — but we’re not — NIH also does the basic, basic, basic cellular first-step science that eventually leads to the work that drug companies do to develop drugs. They do the basic, what they call bench, science.
I’m not hearing the drug companies speak out. The ambivalence Americans have about drug companies, which is hating the prices but liking the drugs, I haven’t heard pharma — Maybe it’s just too early. Maybe they’re weighing in quietly, and maybe Anna can tell me I’m wrong and they are and I just didn’t notice. But that’s also a huge constituency, a huge, powerful constituency. Because without the NIH, we wouldn’t have many of the drugs that keep us and our elderly relatives alive, including a lot of the gains — we haven’t cured cancer, but we’ve made gains on cancer. That wouldn’t have happened. It’s not just the premier research institute in America. It’s the premier research institute in the world, and as Julie said, a big driver economically of every single county, every medical school, every public health, you know, it has been an economic powerhouse as well as a knowledge powerhouse.
Edney: And I wouldn’t tell you you’re wrong. I think that you’re right. I haven’t heard the pharma companies talking about it. I think they are talking about a lot of things that they want done to benefit them, and so I’m sure that they’ve made their priorities. We’ll see if this reaches sort of a boiling point, where they do end up weighing in. And I also just want to say, NIH, I know they want to focus on chronic disease. It does a lot of that. So maybe that’s not being communicated: It’s not being cut or left off the table because we’re doing this. We can do two things. We can walk and chew gum.
Rovner: Yes, I know, and that was the point I was trying to make. It’s like, there’s an enormous amount of chronic disease research that happens from the NIH, much of it dictated by Congress already. They spend a lot of time, individual members, telling NIH what it is they should be studying, which is a whole other issue that we’ll get to another time.
But I want to stay on the topic of drug prices, because that’s a really big question mark for the incoming administration. This week, the CEO of drugmaker Eli Lilly told a Bloomberg reporter that it will ask the Trump administration to, quote, “pause” the Medicare drug price negotiation program, which of course is just getting underway.
Of course, that’s happening even as Lilly encourages the incoming HHS [Department of Health and Human Services] not to cancel a Biden administration decision to have Medicare begin covering its expensive new weight loss drugs.
Meanwhile, on its way out the door, the Biden administration’s Federal Trade Commission dropped a report that found that the nation’s three largest PBMs, which together control about 80% of the U.S. prescription drug market, drove up drug prices by an estimated $7.3 billion from 2017 to 2022.
I saw somewhere this week, and I think, Sandhya, you mentioned this, a suggestion that Republicans might try to resurrect the PBM bill that was dropped from that year-end 2024 spending bill and put it in the next spending bill that Congress is going to have to do in March. Likely? Possible? Will this report have any impact? Or is there just too much other news this week and nobody’s going to remember?
Raman: I think it’s definitely being talked about a lot. We talked to the leadership of Energy and Commerce. It’s a priority for both of them, both for Carter and for Guthrie, because they worked so closely on it before. It was included in a bipartisan deal that we had before we got the CR [continuing resolution] that we voted into law. It just got dropped along the way.
Rovner: When Elon Musk said the bill was too big?
Raman: Yeah. So I think we kind of have two pathways, where both of them want to get it done regardless. I think that it might depend whether they are able to piece it away and do it as something stand-alone, which they want to get it done sooner rather than later.
But it depends a little bit more on the leadership level, if there are savings from using that bill to be used later down the line when they get reconciliation at a later stage. So I think that’s what we’re waiting on. Would they need to put that there? Or would they be able to go forth with that now?
Rovner: True. So, it’s a bipartisanly popular provision that also saves money, so that makes it kind of attractive to lawmakers who are putting together things that might, as Joanne would say, include spinach.
Anna, what more broadly do you see as the outlook on drug prices?
Edney: Well, I think the first thing I think of with that program is, it saves a lot of money if you’re giving Medicare the ability to negotiate. And so, I just wonder how that fits into this agenda if you stop it and make it more favorable towards the drugmakers. Where does that fit in with cutting spending and reducing the deficit and all of those things?
So, I think that, maybe they have a little bit of an uphill battle in making their case on that front. All of this, for me, hinges on whether Trump really means what he says. And I think we all know that we just have to wait and see what actually happens.
Rovner: Yeah, a lot of shrug emojis coming.
Edney: Exactly.
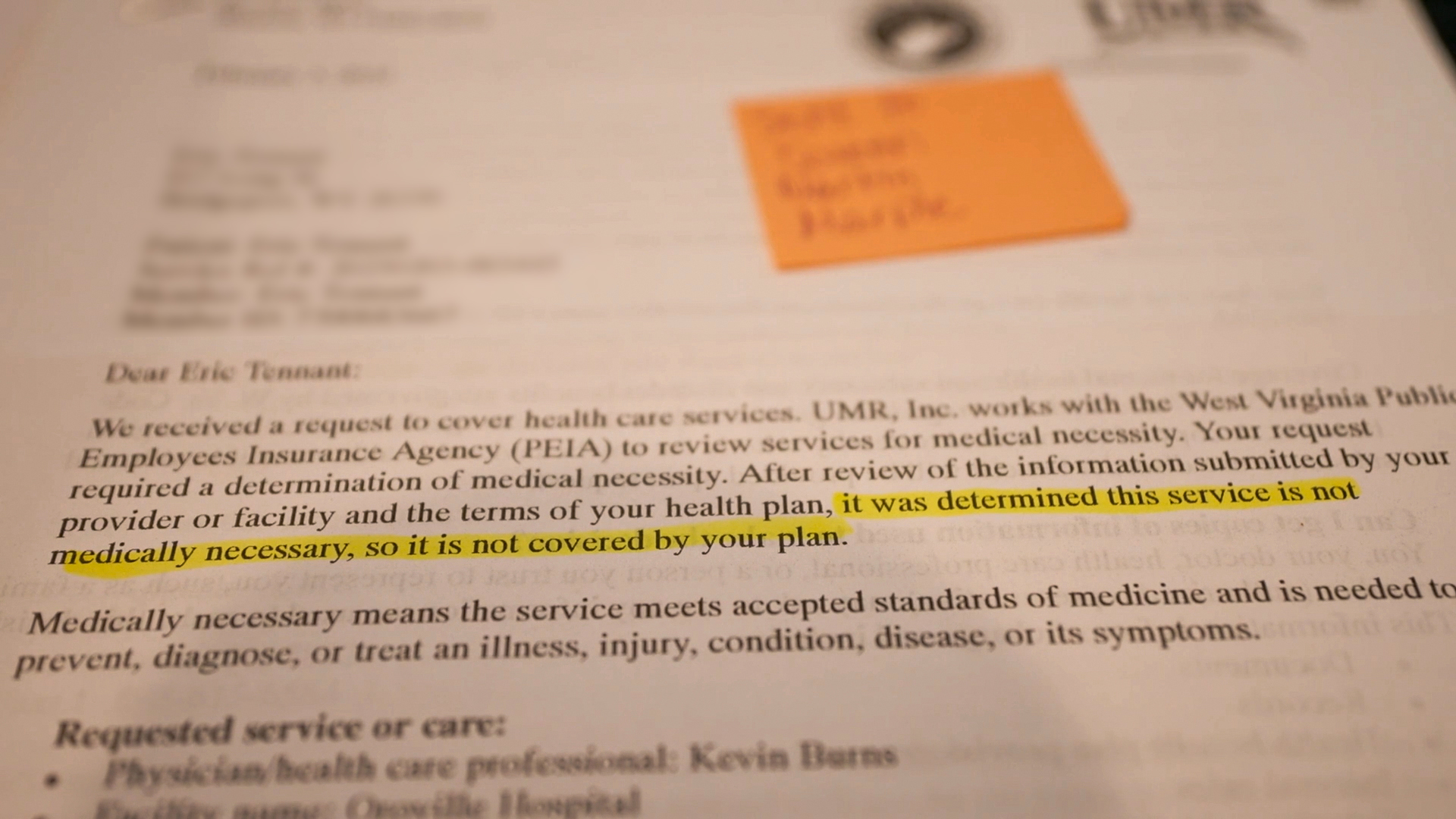
Rovner: Well, meanwhile, across the street from Capitol Hill, the Supreme Court has agreed to hear that preventive health care case out of, altogether now, Texas. The case challenges the requirements in the Affordable Care Act that insurance cover, without copay, preventive services like immunizations, cancer screenings, birth control, and, the subject of this particular case, medication to prevent HIV.
What happens if the court rules with the plaintiffs in this case who argue that the CDC’s [Centers for Disease Control and Prevention’s] Preventive Health Services Task Force does not have the authority to determine what services should be on this list? Which of course is the entity that now determines which services should be on this list.
Edney: Well, it sounds like, then, a lot of people don’t get their preventive care covered. As KFF wrote, there is some that would be still covered, the mammographies, but not the HIV preventative medication. Other cancer screenings included in that as well. And so, it seems to throw a wrench, I guess, sort of just asking this of the panel, that agencies then would have to go make those determinations? Does Congress have to make the determinations on what’s covered then?
Rovner: Well, that’s of course the big question. Or, would the secretary, him or herself? Who is authorized? I think the argument is because the Preventive Health Services Task Force is not Senate-confirmed, they can’t make these decisions.
And of course, the way it works, they don’t make these decisions. They recommend them, and then the secretary sort of ratifies them. So it’s hard to tell from this whether it really would go away, or whether Congress would have to step in, or whether the secretary could just do it. I feel like this creates as many questions as it could answers.
Kenen: It’s a really broad array of benefits that — it’s not just the HIV PrEP preventive medicine. And I read different stories about this, and they had different lists, including some cholesterol stuff. And I don’t know, since the lists were so different, I’m not sure exactly which ones are in or which ones were out. But it’s not just HIV drugs. It’s a lot of stuff.
So it would certainly gut something that people count on now. I mean these are free not just under an ACA plan but if you get coverage through a job, those requirements also apply. So, a lot of people would no longer have free access to a lot of what we consider preventive care.
Rovner: We’ll be watching this case. They have not scheduled oral arguments. They just decided to take it. So, this will be a later in 2025 case. Well, the flip side of an incoming administration are all the things the outgoing administration tries to slip through on its way out of town, and this week has seen a bunch of those.
Most of these things could be fairly easily undone by incoming officials, but not without some public pain, which sometimes is why administrations wait until the very last minute to do them, to be a little passive aggressive, or maybe in some of these cases a lot passive aggressive. Several of these last-minute changes come from the Food and Drug Administration, an agency targeted for big changes under Trump 2.0.
In just the last 48 hours, the FDA has announced a policy that would require dramatic reductions in nicotine in cigarettes to render them, quote, “minimally addictive or nonaddictive.” It moved to ban Red Dye No. 3, a controversial additive already banned in many other countries which has been shown to cause cancer in rodents. And it proposed a major change in food labels to require them to show on the front of packaging whether the food’s sodium, sugar, and saturated fat levels are low, medium, or high. Do any of these proposals live on for more than another week?
Edney: I think the Red No. 3 could. We know that R.F.K. Jr.’s talked about food dyes and wanting to get them out of, he specifically said, cereal, but they’re in a lot of things. So, I see that one.
I think the industry saw that coming from far away and has been switching already, of course sometimes to another problematic, potentially, food coloring. But I don’t think this is something you’re going to see them fight super hard for to change. The nicotine is much more iffy. Big Tobacco is still a huge force, and Trump gets funding for his campaign and things from companies who have a stake in this.
And some of that could align with this idea of not necessarily medical freedom but, sort of, we can choose what we put in our bodies. If we want to be addicted to nicotine, that’s our choice. So, the other one, the labels, I’m not sure. They’re not particularly powerful or anything. I thought they looked … When I looked at it, I was like, This is confusing and just looks like the back, but it is a little different. So, I don’t know. Maybe it survives. I’m not sure how much the industry is working on this.
Rovner: [Sen.] Bernie Sanders of all people excoriated the food labels, saying we don’t put on cigarette packages whether the cancers they cause are low, medium, or high. Why should we do this? I mean, this is basically another effort to go after ultra-processed foods. I was surprised at how angry he was at this.
Kenen: I think he wants them in neon.
Rovner: I think he wants R.F.K. Jr. to have fewer ultra-processed foods available. I think that’s going to be sort of the big takeaway from all of this, I guess.
Kenen: Right. But we also don’t understand what an ultra-processed food is, because there’s some foods that are not ultra-processed that are bad for you. And there’s some foods that do have some kind of minimal processing that, I mean, we’ve come to lump this together and I couldn’t tell you. There’s some things that are, quote, “ultra-processed” that really aren’t that processed, don’t have a lot of additives. They have something.
So the whole categorization needs more work, both for public understanding and political understanding. There’s nobody who’s going to say that Americans have a really healthy diet and that food additives … R.F.K. Jr. has pointed out to the food additive, where the companies have to get to self-certify, Yeah, this is safe. So, is that something that he could get widespread support on? Yes, but there’s a whole lot of other things that he says that people were not going to agree with.
Rovner: And I will remind that we not only don’t know if R.F.K. Jr. will be confirmed, but they still don’t even have a date for his confirmation hearing, because they’re still waiting on the paperwork. All right, moving on.
As we taped this morning, there are still several fires burning in the Greater Los Angeles area. We have talked about the health effects of fire before. It’s not exactly news that fire and smoke are bad for human health, but what seems to make these fires different is that they’re not mostly trees and brush and other bits of nature that are burning but lots of toxic substances that are polluting not just the air but also the drinking water.
Are we going to have to start thinking about fire and health in a much different way if not just remote areas but entire suburbs are now prone to burning up as a result of our changing climate?
Edney: It will make us think of a lot of things in different ways, and particularly health care, when there’s things like high benzene levels floating in the air. We know that so much of our interior environments are made with things that contain high levels of formaldehyde, things like that.
I think the expectation is that can create a long-term issue, but also it can in the moment create more deaths just at the time, not because it directly kills but if you already have an issue and you have a respiratory problem or a heart problem that can be exacerbated by these fires.
Yeah, I think there’s a ton to think about. Even drinking water can be impacted more so when you have power outages and things in the areas where you’re maybe cleaning that water and then things like that. So, I think that’s going to be — masks, N95s might be coming back for a totally different reason.
Rovner: Well, N95s are not enough. I mean, I think that was the thing that kind of jumped out at me. If you watch the news coverage of it, the reporters aren’t wearing N95s anymore. They’re wearing what looked like old-style gas masks. I mean, you need sort of the next level of masking because N95s don’t filter out some of these toxic substances that are now floating in the air. I mean, they do filter out the sort of the actual smoke from wood and whatnot, but it’s pretty scary.
I mean, a lot more people than ever before have N95s hanging around their house, but they certainly don’t have these next-level respirators, which is what I keep hearing doctors calling for.
Kenen: And the article you — I think it was the one that you sent around yesterday that basically that everything in our house is, our couches are basically cubes of plastic wrapped in cloth and dangerous when they’re burned. But I mean, I think that was the article that also said that some of these things that are burning produce like a cyanide kind of gas, that the firefighters can’t even be exposed. They can’t stand in front of a house with a hose for a long time.
It could be killing or injuring firefighters. So, it also hampers — they’re not just trying to put a hose on a burning tree.
Rovner: Yeah. A lot more things to think about, which is just what we needed. Well, turning to abortion, remember all those states last year that voted to protect abortion rights? It seems that was far from the final word.
We are seeing court case after court case to determine which abortion restrictions can stay and which can’t as a result of passage of those ballot measures. This is happening particularly in Missouri, where Planned Parenthood clinics are still not offering the procedure after a judge invalidated some but not all of the state’s restrictions.
This seems to be the inevitable result of what we have seen in other elections, where the same voters endorse abortion rights but then turn around and vote for candidates, including judges, who don’t. Is the gridlock here on purpose or by accident? And Sandhya, what’s going to happen?
Raman: I don’t know that it would be on purpose. I think that these voters that vote for the candidates, if abortion is not their top issue, they’re still going to vote in the way that kind of allies with them. But then if they’re looking at other policies, they’re going to vote for these candidates.
And Missouri, I think, is interesting because it has long been, I think, one of the test cases for so much in the abortion space, of trying out new restrictions and what will stick to the wall. And I think that we’re going to see more of these kind of long, drawn-out battles, given that the judge said that some restrictions were struck down because of the constitutional amendment but then others, like the licensing for abortion facilities, which we’ve seen for years, can stay. And that just makes it so that they can’t really operate.
Rovner: Yeah. They have things like how wide the hallways need to be, I mean, rules that were created to deter them from offering abortions, not because they were actually needed for safety and health.
Raman: Yeah. These rules only apply to the abortion facilities. They’re not parallel in the other types of clinics and hospitals. So it’s targeted to them. I think it is just another example of it being kind of an uphill battle for them, because now, I mean, even in the past few years we’ve seen so much more attention on state supreme court races, which I feel like a few years ago that was not something that would get national attention for one state or another.
But, given that, as they’re kind of litigating these and seeing how can we implement the law so that these clinics can open under the constitutional amendment, it relies on them, and just how much money that is being fueled to be able to not come down on the other side so that they can kind of operate. So I think that’s something to definitely watch, as some of these states are kind of litigating these things, but it’s going to be a long, drawn-out battle, even if it’s already been several months since seven out of 10 states last year voted in favor of abortion rights.
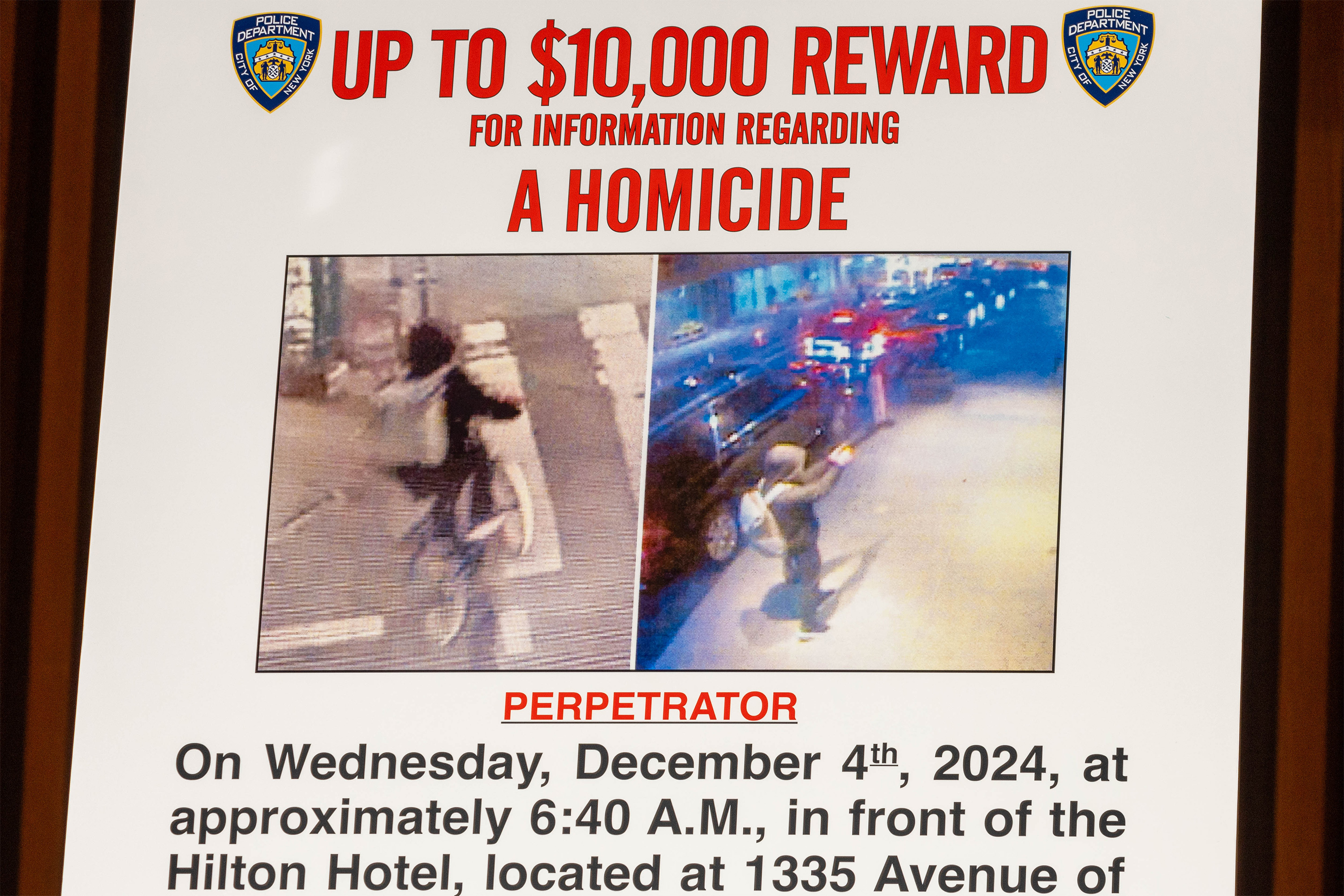
Rovner: Yeah, this continues, and of course, we’ll wait and see what happens at the federal level, when the Trump administration gets going. Well, finally this week, we have another entry in our recurring segment, “This Week in Medical Misinformation.” I wanted to talk about a little-noted story from the medical news site MedPage Today about the American Board of Internal Medicine pulling the board certification of a Texas cardiologist who made controversial and untrue claims about covid and the covid vaccine, including that vaccine had killed tens of thousands of people.
What’s troublesome about this story, though, is that the ABIM wouldn’t comment on individual physicians, although it did list this particular doctor on his website as not being certified. How should specialty boards deal with doctors who express views that are, shall we say, not consistent with medical evidence? And how transparent should they be about telling patients when they sanction one of their own, which is basically what happened here?
Kenen: Well, they did put out a statement, I think it was the New England Journal of Medicine about a year and a half ago, saying that they were going to crack down on this. I’m not sure if there’s, for any of the boards, if there’s a mechanism for telling patients, because how do you even know who all the patients or potential patients are?
Rovner: But when I say telling patients, I mean telling the public.
Kenen: Right. But I don’t know that any of the boards do that in any — it’s a big can of worms about decertification and how infrequently it happens.
So ABIM did put out a statement, I think it was two years ago now, and there’s been a process for a few, but not a lot. And it doesn’t mean they don’t have a license anymore. It means they don’t have board certification. So unless the state medical board, which is really the group that pulls a license — this is saying that you’re not a board-certified whatever your specialty is under ABIM.
But Lauren [Weber of The Washington Post], who is sometimes on the website, had a good piece a couple of months ago about how few state boards have acted to sanction doctors who say incorrect things about vaccines. And that goes back way before covid. The medical profession doesn’t do a lot of self-policing.
Rovner: Yes, and I’ve been doing this long enough to have covered the creation of the National Practitioner Data Bank, when doctors who’d had their licenses pulled could just go to another state, and there was no way for that state to easily find out that that doctor had had his or her license revoked.
And that was usually not for saying things but for doing things that ended up with having the doctor decreed not qualified to practice medicine anymore. So, I mean, this is an issue that goes back a long ways.
Kenen: And you would think they would be the opposite. You would think that the state boards, when somebody is really a bad guy or a bad gal, you would think they would say, “We stop them!” Like, “We are protecting your health.” And instead, it’s been very secretive and very infrequent.
It’s more the state licensing board. I mean, certification is important, but really the power to de-license somebody is in the state boards.
Rovner: Yeah, well, the whole argument that professions police their own, what we’ve discovered is that professions don’t do a very good job of policing their own. But we will keep watching. All right, that is the news for this week. Now, we will play my “Bill of the Month” interview with Harris Meyer. Then we’ll come back and do our extra credits.
I am pleased to welcome to the podcast Harris Meyer, who reported and wrote the latest KFF Health News “Bill of the Month.” Harris, welcome to “What the Health?”
Harris Meyer: Thanks very much, Julie. Glad to be here with you.
Rovner: So, tell us about this month’s patient — who he is, where he’s from, what kind of medical care he got.
Meyer: OK, Julie, this is a story about high prices, confusing bills, and lack of price transparency for a very common procedure. The patient is Tom Contos, a 45-year-old health care consultant who lives in Chicago. Last spring, Tom noticed blood in his stool. He went to see his family physician at Northwestern Medicine.
The doctor referred him for a diagnostic colonoscopy because of the bleeding and because of his family history of serious colon issues. Then in June, he went in for a colonoscopy at Northwestern Memorial Hospital, which is a big teaching hospital in downtown Chicago.
A Northwestern gastroenterologist performed the procedure, which took less than an hour. He found and removed two polyps, which a pathologist later found were not cancerous. The gastroenterologist concluded that Tom’s rectal bleeding was due to a large hemorrhoid.
Rovner: So, just to be clear, it’s screening colonoscopies, those for people with no symptoms, that are supposed to be free as preventive care under the Affordable Care Act. Diagnostic colonoscopies like this one can require a patient to meet deductible and copay requirements, right? That’s something important for people to know?
Meyer: Yes. There’s a lot of confusion about this. I got a lot of comments on my Washington Post article that expressed confusion. Yes, diagnostic colonoscopies like Tom’s are done when there are symptoms like bleeding or pain. In contrast, screening colonoscopies are recommended starting at age 45, even when there are no symptoms, to prevent colon cancer or other serious conditions.
The Affordable Care Act requires health insurers to cover screening colonoscopies at no cost to patients. But for a diagnostic colonoscopy, patients may have to pay a deductible and copayment, even though that procedure similarly can prevent colon cancer. It doesn’t—
Rovner: It can be confusing.
Meyer: It’s confusing, yeah.
Rovner: So he has a procedure, which found some minor indications that were taken care of, and then, as we say, the bill came. How much was it?
Meyer: Yeah, Northwestern’s total charge was a mind-boggling $19,000. Tom’s insurer, Aetna, had a negotiated rate with Northwestern of a still significant about $6,000. When he got his insurance explanation of benefit statement, he saw that he owed about $4,100, with the insurer paying about $2,000.
He was bewildered because he had asked Northwestern for an estimate of how much he would owe in total and he was told that he would owe about $2,400. My outside billing expert said $4,100 is quite a high out-of-pocket bill, though not unusual for teaching hospitals.
Rovner: And he was charged for two colonoscopies, right?
Meyer: Yes. That was a major reason that the bill was so high. Northwestern billed him for two colonoscopies, which Tom did not understand, since he had only received one. It turns out that providers routinely bill for two procedures if the gastroenterologist removes and biopsies two polyps in two different ways during the same procedure.
The second procedure is billed at a discounted rate. Now, this seems strange to laypeople, but this is how providers get paid for the extra work of removing two polyps rather than one.
Rovner: Which, as you pointed out at the beginning, it’s not like this is a several-hour surgery. This is a fairly quick procedure.
Meyer: That’s right. It’s at most an hour, often less than that.
Rovner: So what happened eventually with the bill?
Meyer: Well, Tom appealed the bill to Northwestern and Aetna and was told that it was correct. He had already paid about $2,400 of the nearly $4,100 he owed, but he told Northwestern that its bill was, quote-unquote, “ridiculously high” and he wasn’t going to pay the remaining $1,700 or so and that they could take him to collections.
Northwestern said that’s what they were going to do, and Tom decided to no longer use Northwestern or its doctors in the future.
Rovner: Although I assume he did pay the amount that they said he owed.
Meyer: No, he said: Take me to collections. I’m not paying it. My credit is good, and — I won’t repeat some of the things that he said to them.
Rovner: Thank you. This is a family podcast. How can others avoid falling into this trap? I mean, he got an estimate. He had an idea of what he was going to be charged, and yet he was still charged considerably more than that estimate.
Meyer: Yeah, he’s a health care consultant, but a lot of people get confused by this process, including him taken by surprise. He only looked at the estimate after he had had the procedure but before he got the final bill. So, like a lot of people, he got confused and he didn’t proceed necessarily as efficiently as he might have. But that’s common and not surprising.
Rovner: Even for somebody who’s basically in the health care payment business.
Meyer: Yes, that’s correct.
Rovner: So be vigilant. Is that basically the takeaway?
Meyer: Well, how can you avoid falling in the same trap? Unfortunately, not easily. Patients needing a diagnostic colonoscopy should check out freestanding endoscopy centers or ambulatory surgery centers that aren’t associated with a hospital, because they can be cheaper and they can provide good quality of care.
To price-shop ahead of time, patients can look at the hospital’s price website and their insurer’s cost estimator website to get a sense of how much a diagnostic colonoscopy could cost. They also can look up a so-called good faith estimate of the cash price, meaning the procedure could be cheaper if they pay cash, rather than going through insurance.
Plus, there are free websites such as Turquoise Health and Fair Health for checking prices for colonoscopies and other procedures. Now, once they get a price estimate from the provider, there’s one more wrinkle. Patients should ask whether that price includes the extra services, if the gastroenterologist finds and has to remove and biopsy one or more polyps. At least 40% of colonoscopies do find polyps.
Now, experts say it’s unfortunate that getting a diagnostic colonoscopy can be so expensive and confusing billing-wise, but don’t hesitate, because it can be a lifesaving procedure for many people.
Rovner: All excellent advice. Harris Meyer, thank you so much.
Meyer: Thank you, Julie.
Rovner: OK, we are back, and it’s time for our extra-credit segment. That’s where we each recognize the story we read this week we think you should read, too. Don’t worry. If you miss it, we will put the links in our show notes on your phone or other mobile device. Anna, why don’t you go first this week?
Edney: I wanted to talk about one I wrote last month, and the headline is “It’s Not Just Sunscreen. Toxic Products Line the Drugstore Aisles.” I kind of wanted to put in one place talking about a lot of these contamination issues that have come up, but particularly also just show that, while the problems with products keep growing — one of them that I pointed out that’s new in this piece is dandruff shampoo containing benzene — the FDA is getting sort of slower on a lot of these things. They’re digging in, and they’re not trying to communicate to the public about the issues that have come up. They’ve had since last March of 2024 concerns brought to them about benzene and acne products.
They’ve said nothing to the public. They just keep saying, We’re looking at it. And that’s very different from when this first kind of started happening on a larger scale, where it was like, boom, recalls. Now it’s just sort of this fight to maybe not have recalls. I don’t know what’s going on in their head.
But there also are some issues in there with the tampons were found to contain a lot of heavy metals, FDA also slow-walking there. So I wanted to point out that piece I wrote if anybody missed it.
Rovner: Yes. Thank you, Anna, on the “everything you thought might be safe is actually dangerous” beat.
Edney: I’m the life of every party.
Rovner: There you go. Joanne.
Kenen: I’m not sure if this is an extra credit or a public service announcement, but there is a great piece in The Atlantic by Daniel Engber. Well, we all know there’s a ton of stomach bugs and norovirus going around, and it’s quite severe this year. And the headline is “A Secret Way to Fight Off Stomach Bugs,” and the answer is wash your hands with soap.
But it’s a really well-written — it actually makes you laugh about stomach bugs. It’s a very well-written, good story. And no, for this bug, hand sanitizers don’t work.
Rovner: Sandhya.
Raman: My extra credit this week is called “New obesity definition sidelines BMI to focus on health,” and it’s by Giorgia Guglielmi for Nature. And it takes a look at — we had a revised definition of measuring and diagnosing obesity in the Lancet Diabetes & Endocrinology this week.
So, instead of BMI [body mass index], which is weight- and height-linked, they’re suggesting a couple of alternatives: preclinical obesity, which is a person with extra body fat but their organs are still functioning normally, and clinical obesity, so when you have that excess body fat that it’s harming your organs. And there’s more in the piece on just different ways clinicians are looking at this globally.
Rovner: Yeah, it’s really interesting because, obviously, every doctor says that BMI is a stupid and imprecise way to measure this, and then everybody uses BMI because, at the moment, it’s all we have. My extra credit this week is a KFF Health News story from Felice Freyer. It’s called “Can Medical Schools Funnel More Doctors into the Primary Care Pipeline?” and it’s about a problem I have been following for a while and which does not seem to be getting better.
While the U.S. has opened lots of new medical schools over the past decade and has launched a raft of programs aimed at getting more graduating doctors to go into primary care, way too many are still pursuing specialty care instead. We have tried, as a society, free tuition and loan repayment programs, but it doesn’t seem that medical education debt is the biggest problem.
We’ve also tried training doctors in more primary-care-centric locations, i.e. in community clinics rather than in hospitals, but that’s not made a huge dent, either. Rather, to quote one of the family medicine experts in the story: “It’s not the medical schools that are the problem; it’s the job. The job is too toxic.”
In other words, it’s not really appealing to see too many patients for too little time and do tons of fighting with insurance companies and electronic medical records. Until we as a society start making primary care a lot more of a satisfying job, it’s not going to matter how much it pays. We’re still going to have a serious shortage.
All right, that is this week’s show. As always, if you enjoy the podcast, you can subscribe wherever you get your podcasts. We’d appreciate it if you left us a review. That helps other people find us, too. Special thanks again this week to our temporary production team, Taylor Cook and Lonnie Ro, as well as our editor, Emmarie Huetteman.
As always, you can email us your comments or questions. We’re at [email protected], or you can still find me occasionally at X, @jrovner, and increasingly at Bluesky, @julierovner.bsky.social. Where are you guys hanging out these days? Anna?
Edney: On X, @annaedney, and then on Bluesky, @annaedney.bsky.social.
Rovner: Joanne.
Kenen: I’m on Bluesky, @joannekenen.bsky.social, very occasionally on X still, @JoanneKenen.
Rovner: Sandhya.
Raman: On X, @SandhyaWrites, and on Bluesky, @sandhyawrites.bsky.social.
Rovner: We will be back in your feed next week. Until then, be healthy.
Credits
Taylor Cook
Audio producer
Lonnie Ro
Audio producer
Emmarie Huetteman
Editor
To hear all our podcasts, click here.
And subscribe to KFF Health News’ “What the Health?” on Spotify, Apple Podcasts, Pocket Casts, or wherever you listen to podcasts.